Hemodialysis vs Peritoneal Dialysis.
Hemodialysis vs peritoneal dialysis: understand the differences in schedule, access, risks, and lifestyle impact to choose the right fit.
When kidney failure treatment becomes necessary, the choice between hemodialysis vs peritoneal dialysis is rarely abstract. It affects where treatment happens, how often your week is structured, what type of access procedure is required, and how much flexibility you may have for work, family life, or travel. For some patients, one option is clearly more appropriate. For many others, the correct answer depends on medical stability, home support, infection risk, and personal priorities.
Hemodialysis vs peritoneal dialysis: the core difference
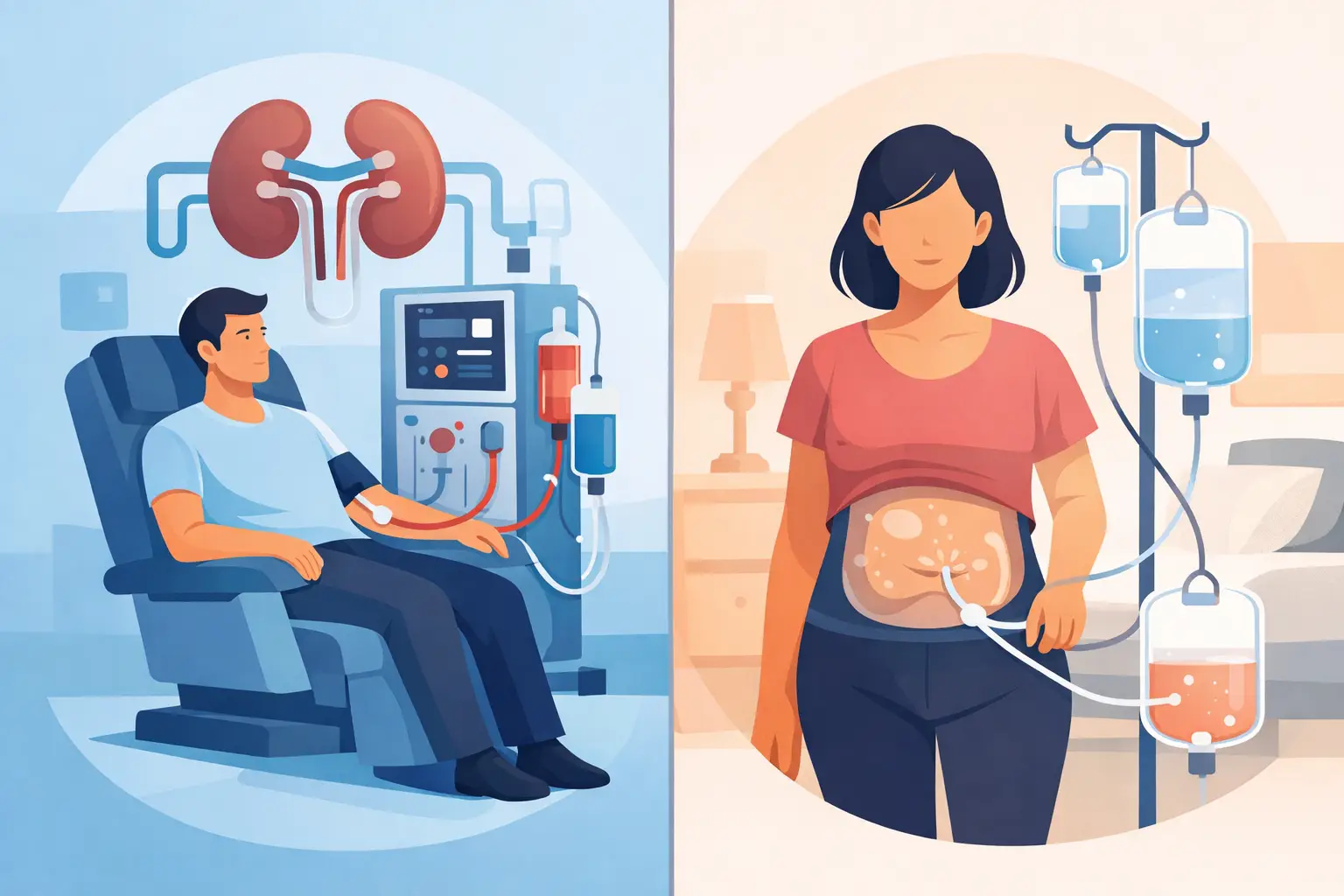
Both treatments replace part of the kidneys' filtering function, but they do so in very different ways. Hemodialysis removes blood from the body through a vascular access, passes it through a dialysis filter, and returns the cleaned blood to the circulation. This is usually performed in a dialysis unit on a fixed schedule, though home hemodialysis is possible in selected settings.
Peritoneal dialysis uses the lining of the abdomen, called the peritoneal membrane, as the filter. Dialysis fluid is placed into the abdominal cavity through a soft catheter. Waste products and excess fluid move across the membrane into that fluid, which is then drained and replaced. This can be done manually during the day or with a cycler machine at night.
The practical distinction is straightforward. Hemodialysis is typically center-based and intermittent. Peritoneal dialysis is home-based and continuous in its overall effect, even though the fluid exchanges occur in cycles.
How hemodialysis works in daily life
Most patients receiving in-center hemodialysis attend treatment three times each week, with each session often lasting about four hours. Extra time is needed for travel, preparation, and recovery. Some patients feel reasonably well afterward. Others experience fatigue, cramps, headaches, or low blood pressure, particularly if a large volume of fluid must be removed.
A reliable access is essential. The preferred long-term access is usually an arteriovenous fistula, created surgically by connecting an artery to a vein. In some cases, an arteriovenous graft is used. A central venous catheter may be necessary for urgent dialysis initiation, but it is generally less desirable for long-term use because infection and clotting risks are higher.
Hemodialysis can be an excellent choice for patients who want treatment supervised directly by dialysis staff and who may not be able to manage dialysis independently at home. It also suits patients whose abdominal anatomy or prior surgeries make peritoneal dialysis less feasible.
How peritoneal dialysis works in daily life
Peritoneal dialysis requires placement of a catheter into the abdomen. After healing, dialysis is performed at home. With continuous ambulatory peritoneal dialysis, the patient performs manual bag exchanges several times a day. With automated peritoneal dialysis, a machine usually performs exchanges overnight while the patient sleeps.
This option offers greater independence for many people. There are no routine needle sticks into a fistula, and treatment can often be integrated more smoothly into employment or travel. Because fluid and waste removal are more gradual, some patients feel more stable from day to day and may experience fewer abrupt post-treatment symptoms.
That said, peritoneal dialysis demands consistency, training, and a clean home routine. The patient or care partner must be comfortable following sterile technique. Missed exchanges, poor technique, or catheter problems can lead to serious complications, especially peritonitis.
Which treatment is more effective?
Patients often ask which is better medically. The more accurate question is which is better for a specific patient at a specific point in time. Both hemodialysis and peritoneal dialysis can provide adequate renal replacement therapy when prescribed correctly and monitored closely.
Effectiveness depends on more than the modality itself. Residual kidney function, body size, dietary intake, fluid gains between treatments, cardiovascular health, and adherence all matter. A patient doing peritoneal dialysis consistently with good residual kidney function may do very well. Another patient with high clearance needs or recurrent abdominal infections may do better on hemodialysis.
Survival comparisons between modalities are not simple. Outcomes are influenced by age, diabetes, heart disease, timing of referral, nutritional status, and access to specialist nephrology oversight. This is why a blanket answer is rarely responsible.
Hemodialysis vs peritoneal dialysis for lifestyle and flexibility
Lifestyle concerns are legitimate clinical considerations. They are not secondary issues.
Hemodialysis offers the structure of a scheduled unit. For some patients, that structure is reassuring. Nursing and technical staff are present, vital signs are monitored, and treatment issues can be addressed immediately during the session. The trade-off is that the schedule can be restrictive, and travel requires coordination with another dialysis center.
Peritoneal dialysis usually provides more control over time. Patients may work more regular hours, avoid multiple weekly trips to a center, and maintain a treatment schedule that is less visible to others. This can be especially valuable for younger patients, caregivers, and those who need greater day-to-day autonomy. The trade-off is that the responsibility shifts toward the home environment. Supplies must be stored, technique must remain meticulous, and complications must be recognized early.
For international travelers, both modalities can be managed, but the logistics differ. Hemodialysis requires advance booking with a facility that can accept outside patients and review clinical records. Peritoneal dialysis may allow greater mobility if supplies and support are planned properly, though international travel with equipment and sterile materials still requires careful coordination.
Risks and complications of each option
No dialysis modality is complication-free.
With hemodialysis, common concerns include low blood pressure during treatment, cramping, fatigue after sessions, vascular access infection, clotting, and in some cases difficulty maintaining durable access over time. Patients with significant cardiovascular instability may not tolerate rapid fluid shifts well.
With peritoneal dialysis, the major concern is infection, particularly peritonitis and exit-site infection. Catheter malfunction, hernias, membrane failure over time, and inadequate dialysis in larger patients can also occur. Some patients gain weight from glucose absorption in dialysis fluid, and blood sugar control may become more difficult in diabetes.
These risks are not merely theoretical. They should shape the decision from the beginning. A patient with repeated bloodstream infections from catheters may need urgent access planning for better hemodialysis delivery. A patient with poor vision, limited manual dexterity, or an unsafe home setup may not be a good candidate for unsupervised peritoneal dialysis.
Who is a good candidate for each?
Hemodialysis is often well suited to patients who prefer facility-based care, need closer treatment supervision, have limited capacity for home procedures, or are not appropriate candidates for a peritoneal catheter. It may also be favored when rapid solute removal is needed or when abdominal conditions make peritoneal dialysis impractical.
Peritoneal dialysis is often attractive for patients who want independence, have a suitable home environment, can follow sterile technique reliably, and value a gentler, more continuous form of dialysis. It is commonly considered in patients who still have meaningful residual kidney function and in those seeking more scheduling flexibility.
Age alone does not determine suitability. Neither does diagnosis alone. A highly organized older adult may excel on peritoneal dialysis, while a younger patient with unstable housing may be safer in a hemodialysis unit.
Questions your nephrologist should address
A proper dialysis discussion should go beyond preference. It should include your heart function, blood pressure pattern, abdominal surgical history, infection risk, home support, work demands, travel needs, and long-term vascular access planning. If you are approaching kidney failure, the timing of preparation matters. A fistula takes time to mature. A peritoneal dialysis catheter also requires planning, training, and healing time.
This is where specialist-led evaluation changes the quality of the decision. In a physician-directed renal practice, the conversation is not limited to the machine or the schedule. It includes emergency intake pathways, access readiness, hospital coordination, and whether your current medical condition allows a safe start on the chosen modality.
At a practical level, patients should ask what can go wrong with each option, what support exists if problems arise after hours, and whether the chosen approach still fits if work, travel, or health status changes. Dialysis decisions are not always permanent. Some patients transition from one modality to the other over time.
The right choice is the one that fits your clinical reality
The decision between hemodialysis vs peritoneal dialysis should not be framed as a contest with one universal winner. The better treatment is the one that matches your medical needs, your support system, and your ability to sustain it safely over time. In Jamaica, where continuity, specialist oversight, and treatment logistics can strongly affect outcomes, a careful nephrology assessment is especially important.
If you are facing this decision now, ask for a modality review that is specific to your case rather than general advice. The right plan should make medical sense on paper and hold up in real life, on an ordinary week, with your actual health, your actual home, and your actual responsibilities.
Need Professional Guidance?
Dr. Roger Smith and the team at Renal Services Limited offer comprehensive consultations, laboratory review, and personalized kidney education programs in Jamaica.